Omega-3 EPA vs DHA: Understanding the Differences
**Meta Description:** Learn the truth about omega-3 EPA vs DHA differences and discover which ratio matches your health goals—backed by science, not marketing hype. --- You've been standing in the supplement aisle for ten minutes now, holding tw...

D.C.
Doctor of Chiropractic
Founder of FormulaForge. Doctor of Chiropractic revolutionizing nutritional supplements to be what we all wish they were — real quality, scientifically validated, with the exact ingredients and dosages we choose.
View Full ProfileReviewed by Dr. Brennan Commerford, DC
EPA and DHA are chemically distinct omega-3 fatty acids with fundamentally different functions in the body. EPA drives anti-inflammatory pathways and cardiovascular support; DHA is a structural component of brain and retinal tissue. Most commercial fish oils use generic ratios that match no particular health goal. This guide explains the molecular difference, maps the right EPA:DHA ratio to specific clinical applications, and explains why molecular form — not just total omega-3 count — determines whether you are getting therapeutic value or expensive oil.
Two Molecules, Not One

When patients came to my practice asking whether they should take fish oil, the first question I asked was almost never the one they expected: "What are you trying to accomplish, and do you know the EPA:DHA ratio on your current bottle?" Most did not. And that omission was precisely the problem.
The supplement industry has trained consumers to look at one number — total omega-3 content. "2,000 mg of Omega-3s" reads well on a label. But EPA and DHA are not the same molecule with the same function. They are structurally distinct compounds that behave differently in the body, concentrate in different tissues, and produce different clinical effects. Treating them as interchangeable is not an oversimplification — it is the reason so many fish oil users report no benefit at all.
The research on omega-3 fatty acids has become specific enough that form selection now drives clinical outcomes more than dose selection. The ratio you choose should follow directly from your health goals — not from what happened to be on sale at the pharmacy.
The Molecular Difference That Changes Everything
EPA (eicosapentaenoic acid) carries 20 carbon atoms. DHA (docosahexaenoic acid) carries 22. This structural distinction creates dramatically different biological behavior. EPA functions primarily as a precursor to anti-inflammatory signaling molecules — it converts into resolvins and protectins that actively resolve inflammatory processes throughout the body. DHA, by contrast, is a structural molecule: it becomes part of the phospholipid bilayer of cell membranes, especially in the brain and retina, where it influences membrane fluidity, receptor function, and neuronal signaling.
EPA remains largely active in the bloodstream and peripheral tissues. DHA concentrates in the brain — comprising roughly 97% of omega-3 fatty acids in central nervous system tissue — and in the retina, where it makes up approximately 60% of the polyunsaturated fatty acid content. These molecules are not backup systems for each other. They serve distinct purposes in distinct locations.
Your body can convert EPA to DHA, but at less than 5% efficiency in most adults. If your health goal requires DHA — cognitive support, pregnancy, vision — you must supplement DHA directly. Relying on conversion from a high-EPA product will leave you consistently short.
EPA: The Anti-Inflammatory Specialist
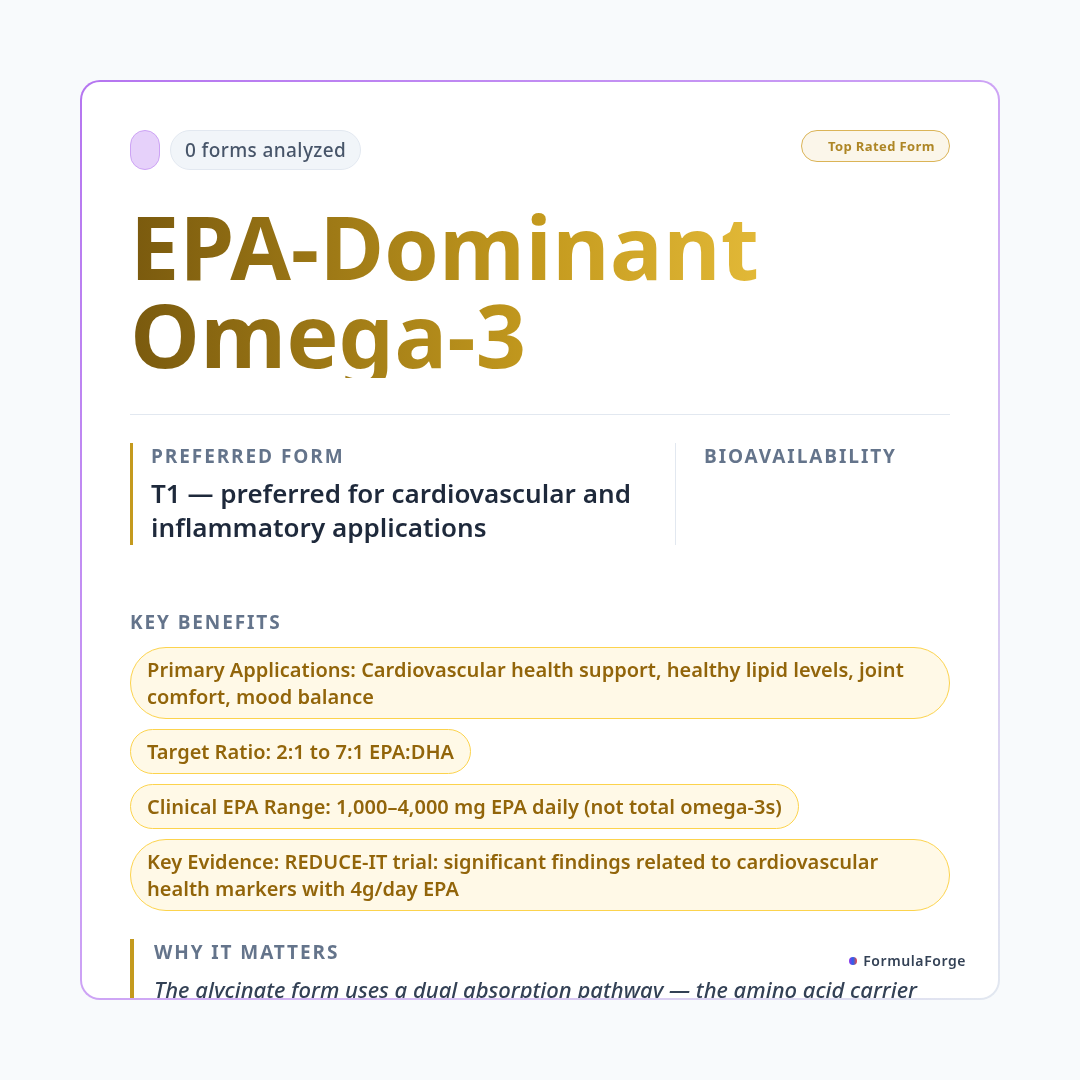
The case for EPA in cardiovascular and inflammatory applications is now one of the strongest in omega-3 research. The REDUCE-IT trial — using 4 grams daily of purified EPA — found a significant findings related to cardiovascular health markers compared to placebo in patients with elevated triglycerides and existing cardiovascular risk. This was not a mixed fish oil study. It was isolated EPA, demonstrating what this specific molecule does when delivered at therapeutic concentrations.
EPA's anti-inflammatory mechanism works through competitive inhibition. It competes with arachidonic acid — a pro-inflammatory omega-6 fatty acid — for the same enzymatic pathways. When EPA is present in sufficient concentration, the body produces fewer inflammatory eicosanoids and more inflammation-resolving mediators. This makes EPA EPA may support healthy inflammatory response and cardiovascular function as part of a healthy lifestyle.
For mood support, a 2019 meta-analysis in Translational Psychiatry examined 26 clinical trials and found that EPA-dominant formulations — with EPA:DHA ratios of 2:1 or higher — showed significantly better outcomes for depressive symptoms compared to DHA-dominant or balanced products. The hypothesis is that EPA's anti-inflammatory action specifically addresses the inflammatory subtype of depression, which is increasingly recognized in clinical psychiatry.
Best for: Supporting healthy lipid levels, cardiovascular function, healthy inflammatory response, joint comfort, mood balance, and metabolic syndrome.
DHA: The Brain's Structural Building Material
DHA's role is fundamentally different from EPA's. It does not drive signaling cascades — it becomes the architecture. When you supplement DHA, it gets incorporated directly into neuronal cell membranes, where it determines how fluid and responsive those membranes are. This structural role means DHA supports cognitive function by changing the physical properties of brain tissue rather than by triggering a particular downstream pathway.
This distinction matters clinically. DHA deficiency does not produce acute inflammation the way EPA deficiency might impair inflammatory resolution. Instead, it produces gradual structural change: membranes that are less fluid, receptors that are less mobile, synaptic transmission that is subtly less efficient. The consequences accumulate slowly — cognitive decline, reduced visual acuity, developmental delays in infants whose mothers were DHA-deficient during pregnancy.
Research published in Alzheimer's & Dementia found that higher blood DHA levels were associated with better cognitive health outcomes in observational research. A 2020 study in Prostaglandins, Leukotrienes and Essential Fatty Acids found that children born to mothers with higher DHA status during pregnancy scored higher on cognitive assessments at age seven. The brain's preference for DHA does not diminish in adulthood — it continues to incorporate DHA throughout life.
Best for: Cognitive support and memory, brain health, pregnancy and fetal development, infant development, visual health, and aging adults with neurological goals.
Molecular Form: The Factor That Determines Whether You Absorb Any of It
Choosing the right EPA:DHA ratio is only half the equation. The molecular form of the omega-3 determines whether your body can actually absorb what the label claims. This is the detail most brands are incentivized not to explain clearly.
Most affordable fish oils use ethyl ester (EE) form — a synthetic form produced during concentration. Ethyl ester omega-3s require an additional enzymatic step for absorption, and research shows their bioavailability is 20–50% lower than natural triglyceride forms. A product claiming "1,000 mg EPA" in ethyl ester form may deliver only 500–800 mg of that to your bloodstream.
Re-esterified triglyceride (rTG) form provides roughly 124% better bioavailability compared to ethyl ester, according to research in the Journal of Nutritional Science. Natural triglyceride form, found in whole fish oil, also outperforms ethyl ester significantly. Phospholipid form (from krill oil) also offers excellent absorption. Always check the label for form specification.
This is not a minor pharmacological detail. A patient taking 2,000 mg daily of an ethyl ester fish oil may be absorbing the equivalent of a 1,000–1,600 mg triglyceride product. If therapeutic dosing for their goal requires 2,000 mg of actually absorbed EPA or DHA, they are consistently falling short — and attributing the failure to fish oil not working, rather than to form selection.
Matching the Ratio to the Goal
These are not arbitrary ranges. Each recommendation traces to the clinical trial literature for that specific indication. The REDUCE-IT data supports high-EPA ratios for cardiovascular applications. The Alzheimer's and cognitive literature consistently implicates DHA as the critical variable for brain outcomes. A product with an undefined or generic 3:2 ratio optimizes for none of these goals.
A label claiming "1,000 mg Fish Oil" might contain as little as 180 mg EPA and 120 mg DHA — meaning you would need to take 6 to 10 capsules daily to reach a therapeutic cardiovascular dose. Always read the Supplement Facts panel for actual EPA and DHA milligrams, not total omega-3 content or total fish oil weight.
How FormulaForge Approaches Omega-3 Selection
Every omega-3 formulation in the FormulaForge system is classified by its EPA:DHA ratio, molecular form (triglyceride vs. ethyl ester), and clinical indication tier. When you analyze a supplement label at myformulaforge.com, the system identifies not just whether your product contains omega-3s, but whether the specific ratio matches your stated health goals and whether the molecular form supports the bioavailability the label implies. If you are in a multi-supplement stack, it also checks for duplicate or competing omega-3 sources across all your products — a common issue in patients stacking fish oil with a multivitamin and a greens powder that each include omega-3s.
Evaluating Any Omega-3 Product: Four Questions
Whether you are evaluating a FormulaForge product or any other brand, these four questions determine whether an omega-3 supplement is worth taking at the dose specified:
1. Does the label specify actual EPA and DHA milligrams? Not "total omega-3s" — individual EPA and DHA amounts. If not, the amounts are likely too low to mention, or the manufacturer does not want you to calculate the dose you would need.
2. Does the ratio match your health goal? Use the table above. A balanced 1:1 ratio does not serve someone with high triglycerides. A high-EPA ratio does not serve someone prioritizing cognitive health.
3. What is the molecular form? Look for "triglyceride form," "rTG," or "re-esterified triglyceride." Products listing "omega-3 ethyl esters" are the lower-bioavailability option. Krill oil specifying phospholipid form is also well-absorbed.
4. Is third-party testing documented? Purity certificates verifying actual EPA/DHA content, heavy metal testing, and oxidation levels should be publicly available for any serious omega-3 product. If a company will not show you their Certificates of Analysis, assume the quality is not what the label claims.
The FDA recognizes omega-3 fatty acids as generally safe at doses up to 3 grams per day from supplements for most adults. Higher doses used for triglyceride reduction (up to 4 grams) are available in prescription-grade formulations and should be used under physician supervision. At higher doses, omega-3s have mild blood-thinning effects — patients on anticoagulant medications, those scheduled for surgery, and those with clotting disorders should consult a physician before using therapeutic doses. Rancid fish oil can cause GI distress and provides no benefit; always check oxidation levels and expiration dates.
Frequently Asked Questions
EPA and DHA are different molecules with different functions and different clinical applications. EPA drives anti-inflammatory resolution and cardiovascular protection; DHA builds and maintains brain and retinal structure. Most commercial fish oils offer a generic ratio that serves neither goal particularly well. If you are taking omega-3s for a specific reason, your product should specify the actual EPA and DHA milligrams, use a form with established bioavailability, and deliver a ratio supported by clinical research for your stated goal. Anything less is marketing, not medicine.
This article is intended for educational and informational purposes only and does not constitute medical advice. The information provided here is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or other qualified health provider with any questions you may have regarding a medical condition or supplement regimen. These statements have not been evaluated by the Food and Drug Administration. Dietary supplements are not intended to diagnose, treat, cure, or prevent any disease.
- Bhatt DL, et al. Cardiovascular Risk Reduction with Icosapentaenoic Acid for Hypertriglyceridemia (REDUCE-IT). N Engl J Med. 2019;380(1):11–22.
- Sublette ME, et al. Meta-Analysis of the Effects of Eicosapentaenoic Acid (EPA) in Clinical Trials in Depression. J Clin Psychiatry. 2011;72(12):1577–1584.
- Dyall SC. Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Front Aging Neurosci. 2015;7:52.
- Yurko-Mauro K, et al. Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimers Dement. 2010;6(6):456–464.
- Visioli F, et al. Omega-3 Fatty Acids and Cardiovascular Disease: Accumulating Evidence. Atherosclerosis. 2019;283:187–194.
- Dyerberg J, et al. Bioavailability of marine n-3 fatty acid formulations. Prostaglandins Leukot Essent Fatty Acids. 2010;83(3):137–141.
- Hibbeln JR, et al. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood. Lancet. 2007;369(9561):578–585.
- Lalia AZ, et al. Influence of omega-3 fatty acids on skeletal muscle protein metabolism and mitochondrial bioenergetics in older adults. Aging (Albany NY). 2017;9(4):1096–1129.

Related Research
- ResearchAshwagandha (Withania somnifera) Root Extract — Forms, Dosing & Research(1 form)
- ResearchKrill Oil (Phospholipid-Bound EPA/DHA) — Forms, Dosing & Research(1 form)
- ResearchAshwagandha Root Powder (Whole Root) — Forms, Dosing & Research(1 form)
- ResearchOmega-3 EPA/DHA (Triglyceride) — Forms, Dosing & Research(1 form)